DISEASE &
TREATMENTS
Click to know more about neurological disorders and diseases and it's treatment.
Cerebrovascular Disorders
Majority of the cerebrovascular lesions inchildren are asymptomatic and only found incidentally or at autopsy, so theincidence of these malformations is unclear. There are five major categoriesaccording to the patho-anatomic characteristics viz.
Telangiectases
Venous Malformation
CavernousHaemangiomas
Arteriovenous Malformations(AVMs and Aneursyms)
Moya Moya disease
Haemangioma[Capillary Telangiectasias]
Theseare vascular malformations composed of dilated capillaries with normalintervening neural tissue. Microscopically they contain ecstatic blood vesselswith thin capillary walls. Presence of brain parenchyma between the vascularmalformations distinguishes it from cavernous malformations.
Telangiectasiashave a prevalence of 0.06% to 0.4 %. They are most commonly located in pons butmay occur elsewhere. They are often solitary but multiple lesions are alsodescribed. These lesions may coexist with sporadic or Syndromic central nervoussystem malformations such as Osler-Weber-Rendu disease ( hereditary hemorrhagictelangiectasia) , Ataxia-telangiectasia, or Wyburn-Mason syndrome.
Haemangiomas are rarely symptomatic and often incidental autopsyfinding. The symptoms associated with telangiectasias are hemorrhage seizurescranial nerve palsy extrapyramidal disorders, and focal hemispheric syndromes(secondary to hemorrhage, ischemic necrosis, or progression of lesion). Thosedetected no surgical treatment is required except close observation.
VenousMalformations [Vein of Galen Malformations VGM]
Steinheildescribed in 1895 by, as high-flow lesions leading to cardiac failure , presenting with hydrocephalus.Veinof Galen malformations are rare vascular anomalies in children,. About 30% ofVGM present in neonatesThe vein of Galenis formed embryonically at the age of 3 months with confluence of the medianprosencephalic vein of Markowski and internal cerebral veins and basal veinsposteriorly and is the collecting vessel for a large group ofveins coming from the deep, medially located areas of the diencephalon, basalganglia , midbrain, medial deep thalamic nuclei, medial occipital and temporallobes, and the superior cerebellar surface. It is formed by the joining of thetwo internal cerebral veins with the basal veins of Rosenthal, and continues asstraight sinus when joined with the inferior sagital sinus Remnants ofprimitive arteriovenous connections that persist are hypothesized to accountfor the various malformations. Since the vein of Galen is not attached by duralstructures, it can dilate enormously, and the walls can becomes thick and toughin response to increased flow, pressure and turbulent flow.
Neonateswith a vein of Galen malformation can develop progressive high output cardiacfailure with signs of progressive high output preload heart immediately afterbirth. Infants often present with an enlarged head circumference, pansystolicintracranial bruit, prominent veins around eyes and forehead, and a fullfontanelle. Mild hydrocephalus is thought to be secondary to venoushypertension from high flow shunting, and not from aqueductal stenosis. OlderChildren often have deep midline shunts. Typical symptoms include chronicheadaches, learning disabilities, seizures and, rarely, SAH.
CT withor without contrast demonstrates parenchymal calcifications from long-standingischemia secondary to venous hypertension. MRI is investigation of choice andvery useful to delineate the malformation in relationship to normal brainstructures. MR angiography can define the type of malformation present. DSA isthe definitive study required to define the complex vascular anatomy, the majorarterial supply, and assist with prognosis and planning for the besttherapeutic approach.
Treatment
Endovasculartechniques have revolutionized the treatment. Aggressive stabilization of thecardiovascular function is done. Endovascular intervention is effective incomplete obliteration of these lesions. Presently surgery for vein of Galenmalformations is reserved for those cases with hydrocephalus and patients inwhom endovascular treatment is not possible and when there is a true AVMleading to VGM A subgroup of patients treated for malformations with persistentfistula can be advised streotactic radiosurgery.
Survival rates range from 70% to 80% across all types, with a 50%survival rate in neonates with heart failure. Combined endovascular/surgicaltreatments have improved outcomes, but morbidity and mortality of this diseaseremains high. Outcome is poor for patients whose initial scans show pronouncedhydrocephalus or cerebral atrophy.
Cavernousmalformations [Cavernoma,or Cavernous haemangiomas]
Cavernousmalformations compose a large population of angiographically occult vascularmalformations. These lesions are known to occur anywhere in the neuraxisincluding on cranial / spinal nerves. They constitute 8% to 16% of all cerebralvascular malformations and have incidence of 0.4% to 0.5%. They occurthroughout life but most lesions become symptomatic in adults in their 20s and30s with equal sex distribution. They are predominantly located insupratentorial region and are asymptomatic in most of children.
A cavernoma is a well-defined discrete lesion with “Mulberry like” darkred or purple color surrounded usually by gliotic tissue discolored by previoushemorrhages. It is hypothesized that the growth results from rupture ofthin-walled vessels,and growth of new vessels as part of hematoma organizationleading to production of fibrous scar tissue.
Thecavernoma presents as Sporadic and Familial form. About 40% and more patientsof familial variety are asymptomatic with the autosomal dominant segregationpattern. Genetic abnormalities have only been recently identified.
Neuroimaging
Theyappear on CT as hyperdense or heterogonous lesions, which may enhance oncontrast administration. Calcified lesions are picked up well. MRI is the mostsensitive and specific method for imaging of cavernomas. Characteristic findinghyperintense signal centrally with reticulated pattern; a popcorn or honeycombappearance, and hemosidrin ringsuggestive of repeated hemorrhage. Angiography: has a limited role, only torule out the presence of any vascular malformation and for detection ofassociated angiomas. The most common presenting feature in children withcavernoma is seizures. Seizure,hemorrhage, or progressive neurological deficit is the typical symptoms thatlead to detection of cavernoma. Most episodes of bleeding are minor, and manytimes may occur undetected. Fatal hemorrhages have been reported in cases ofmalformations located in the posterior fossa. More of cavernoma are now detected incidentally in neuroimaging done for otherreasons.
Treatment
Regular follow up is required in all patients with asymptomatic /incidentally detected, multiple lesions and with strong family history bySerial regular neuroimaging. The indication for surgery includes intractableseizures, refractory to medical therapy. Excision of hemosidrin-stained brain /gliotic tissue is done in children with intractable seizures.
ArteriovenousMalformations
AVMs arethe vascular abnormlities consisting of fistulous connections of arteries andveins without normal intervening capillary beds. Thus forms low-resistanceshunts and redirect blood into the venous system, often at high pressures andflow rates. The majority of AVMs are located in the supratentorial region. Lesscommon sited are cerebellum, brainstem and within the ventricle. Only about 2%of the lesions are multiple thus vast majority are solitary. They affectequally in both the sexes with a prevalence of 0.1% in the population. Howeveronly about 12% of these lesions become symptomatic. AVMs have three primary components: feedingartery, nidus, and a draining vein. Venous drainage from AVMs can be eithersuperficial or deep venous system.
ClinicalFeatures
Intracranial/intraventricularhemorrhage is the most common cause of symptoms experienced by children. Inchildren the commoner mode of presentation is hemorrhage (79% of pediatriccases present with hemorrhage), AVMs also presents with seizures, hemorrhage,focal neurological deficit or atypical chronic headache, high-output heartfailure in infants. The pathogenesis for ischemic symptoms is multifactorialincludes vascular steal phenomenon and venous hypertension. The annual rate ofhemorrhage from AVM is 2% to 4% per year.
Imaging
CT scan or MRI scan identifies intracranial hemorrhage, cerebralswelling and/or hydrocephalus MRI also is useful in assisting the neurosurgeonin determining the location of the nidus and helpful in the planning of surgery.MR Angiography or CT Angiography also gives details of abnormal vasculature.However the gold standard remains 4-vessel cerebral angiography as it’s adynamic study and gives fine resolution of the cerebral vessels along withdocumentation of associated aneurysms, venous varices and vasculopathicstenotic segments in arteries and veins.
Treatment
The management of arteriovenous malformations (AVM) continues to evolve.Multimodality treatment including surgery, endovascular therapy andradiosurgery is the current standard of care. The optimal treatment forintracranial AVM is complete surgical excision of the AVM.A post-treatmentangiogram is done to confirm complete obliteration. Radiosurgery is most usefulfor small AVMs in surgically inaccessible areas of the brain, eloquent areas,deep AVMs of basal ganglia, brain stem or to treat residual portions of thenidus after surgical resection. Also children who are not medically unfit forsurgery. The favorable features of AVM for radiosurgery are low flow, compactnidus - volume < 10 cc. Although the treatment is associated with minimalrisk, there is no change in the risk of hemorrhage until the AVM has beencompletely obliterated and the process of nidus obliteration followingradiosurgery can take up to 2-3 years. Approximately 80% of small AVMs will beobliterated 2 years after treatment. Endovascular treatment occasionally usedas the sole treatment, but risk of recurrence remains. It is best utilized asan adjunct to surgery, either to reduce high flow AVMs or to devascularize AVMsto reduce surgical risk.The prognosis for symptomatic AVMs is less favorablefor children due to the increased incidence of hemorrhage. The primaryhemorrhage is fatal in 5% of cases. Rebleeding occurs in 28% of pediatric AVMsand is associated with a poorer prognosis. The mortality rate with rebleedingis 25%, regardless of treatment method. Inspite above figures, postoperativelymotor, speech and cerebellar deficits can improve greatly, and 70% of childrenwith AVMs are expected to be neurologically intact after surgery.
Aneurysms
Aneurysmsare localized, abnormal dilations of blood vessels, usually arising fromarteries. True aneurysms involve all vessel-wall layers, viz Atherosclerotic,syphilitic and congenital aneurysms. A false aneurysm, or pseudo aneurysm, isan extravascular hematoma in communication with the intravascular space thathas been confined by adventitia or “walled off” by fibrous tissue, a processoften incorporating the entire circumference of the vessel. False aneurysms arecommonly found at leaks from the junction of a synthetic graft with a naturalartery, as well as in moyamoya disease.
Ruptureof saccular cerebral aneurysms is the most common cause of nontraumatic SAH inchildren. About 12% of all aneurysmsoccur in children. with 80% of patients presenting in the second decade oflife. Pediatric aneurysms most frequently occur in the middle cerebral orvertebrobasilar arteries Aneurysms in the MCA distribution tend to occur atmore peripheral sites Multiple aneurysms are uncommon in children, occurringonly in 4% to 5% of patient Multiple aneurysms in children more often areencountered with other conditions, such as moyamoya disease, AVM, fibromusculardysplasia, sickle cell disease and following cranial irradiation. Saccularaneurysms diameters greater than 25 mm in diameter are considered giantaneurysms and constitute a larger proportion of aneurysms seen in children ascompared to adults. These may present with symptoms of a space-occupyinglesion.
SAH isthe most common initial presentation: a sudden onset of a severe headache,associated with vomiting, irritability and seizures. Some times alsounconsiousness.10 to 15% of children may have a less severe initial headache,termed a sentinel bleed, prior to the presenting symptoms. Focal neurologicalsigns due to mass effect from the expanding aneurysm can be transient..One-third of children with intracerebral aneurysms have signs of intracranialhypertension, gaint aneurysms presents with symptoms of a space-occupyinglesion.
Anoncontrast CT scan should be performed to evaluate for subarachnoid blood. CTalso is useful to evaluate for hydrocephalus, cerebral swelling andintraparenchymal hematoma. If the imaging or CSF analysis demonstrate evidenceof a SAH, 4-vessel cerebral angiogram should be obtained,
Treatmentof Aneurysmal SAH
The riskof rebleeding is highest in the first 24 hours after initial hemorrhage. Forthis reason, surgical treatment should be scheduled without delay. In very illchildren (high Hunt and Hess grade), surgery may be postponed to allow theircondition to stabilize.
Medicalmanagement consists of hemodynamic stabilization, ICP control and seizureprophylaxis. Endovascular techniques has revolutionized the management withcoiling the aneurysm sac, its expensive but is now available at more and morecenters. Direct surgical clipping of the aneurysm is also done Other techniques Trapping, Wrapping, Aneurysmectomy and Extracranial-intracranial vessel bypass.
The mortality rate for intracranial aneurysm after the first SAH rangesfrom 11% to 20% in children, compared to 20% to 30% in adults. Rates forrebleeding also are lower in children, ranging from 7% to 13%, while in adultsthe rate of rebleeding is approximately 20%. In children, the mortality ratefollowing rebleeding is 25%.
Moya Moya Disease
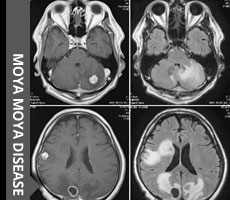
Moyamoya term was introduced Suzuki &Takaku in 1969. The term means “puff of smoke” in Japanese described on theangiographic appearance of the cerebral
collateral network due to the cerebralarteriopathy in children.Its incidence is particularly high in Asia particularily Japan,korea but it has been reported throughout the world.Its onset is often marked by ischemic symptoms in childhood and haemorrhages inadults.
This condition consists in progressivestenosis of both terminal internal carotid
arteries in their supraclinoid part, withthe development of a collaterals network from external carotid supply. It affects3/100 000 children/year with two-third have residual impairment and one fifthwith a recurrence symptoms.
Moyamoya disease is of idiopathic aetiologyand Moyamoya syndrome is secondary to the Congenital [Congenital heart disease,Downs syndrome, Neurofibromatosis, Sickle cell anaemia] or Acquired [Postirradiation ,Post infectious]
Natural history of Moyamoya disease is withgradual stenosis of distal ICA’s, leading to enlargement and proliferation oflenticulostriate and thalamostriate vessels and transdural, leptomeningeal andpial collateral vessels and later Complete collateral and ICA occlusion, reliance on extracranialsources. Mortality can be upto 20% with permanent Neurological sequelae seen in75% and cognitive impairment in half the population.
MRI is investigation of choice recognize theinfracts and ischemic changes ,the tortuous appearance devoid of a signal withT1 weighting and the moth-eaten
appearance of the brain stem nuclei,showing the presence of telangiectases of the moyamoya network. MRA (magneticresonance angiography) not only allows a carotid stenosis to be seen, but also transdural anastomosiscan be identified . DSA has been the gold standard for the diagnosis of the Moyamoya but MRA is replaced DSA as investigation.
Aim of surgical treatment to have revascularisationis prevent stroke & preserve cognition.
Indication for surgery is
1. Occlusive cerebralarteriopathy,
2. Symptomatic cerebral ischemia/cognitivearrest or
3. Decline and Hypoperfusion of uninfected brain.
Revascularisation procedures consists ofdirect and indirect anastomosis
Direct Anastomosis include superficialtemporal Artery anastomosed to the middle cerebral artery
Indirect Anastomosis viz.
EMS (Encephalo-Myosynangiosis)
EDAS (Encephalo -Dural-Arteriosynangiosis)
EDAMS (Encephalo -Dural-Arterio-Myo-synangiosis)
Multiple burr holes
Therefore, moyamoya disease must be knownto pediatrician, neurologist becauseof the multiple clinical features, from ischemic to hemorrhagic strokes, andbecause there is a possible preventive surgical treatment with brainrevascularization.
Click to know more about neurological disorders and diseases and it's treatment.






© 2016 ChildNeuroSurgeon.com. All rights reserved | Design by MHI