DISEASE &
TREATMENTS
Click to know more about neurological disorders and diseases and it's treatment.
The term "Spina Bifida" applies to a failure ofthe spinal cord and spinal column to form properly before birth. This failurecan occur anywhere from the head to the tailbone, but is more common in thelumbar spine. It can occur with a wide range of severity. Spina Bifida Occultais usually found incidentally and is often of no consequence. Myelomeningoceleis a form of Spina Bifida in which the spinal cord is exposed to air at birth.Between these two extremes are other forms, each with its own characteristics
What is a Tethered Spinal Cord Syndrome?
Tethered spinal cord syndrome is a condition caused by abnormal tissueattachments that restrict the movement and ascend of the spinal cord withinthe spinal column. With the spinal column growing spinal cord stretches beyondits tolerance which can then result in lower spinal cord dysfunction due to thedamages of nerve cells and nerve fibers. Tethered spinal cord syndrome may goundiagnosed until late childhood, when sensory and motor problems and loss of bowel and bladder control emerge. Disorders which can lead to tethered cordsyndrome include:
Myelomeningocele
Lipomeningocele and spinal cord lipoma
Dermal Sinus Tracts and dermoid
Diastematomyelia or split cord malformation
Neuroentric syst
How is Tethered Cord diagnosed?
Almost all spinal dysraphism have Neurocutaneous marker viz midlinedimples, sinuses or tracts leading the skin toward the spinal cord, birthmarks, hairy patches, skin discoloration, skin tags or fatty lumps. Its Nature’sway of warning the clinician that some thing wrong with the development ofspinal cord. The most common signs of tethered cord syndrome include loss ofbladder or bowel control and/or loss of function in the legs. The symptoms andsigns of a tethered cord are not always obvious and may result in a delayeddiagnosis. The neurological defect that results from abnormal stretching of thespinal cord may not be reversed by surgery, so it is important to diagnose thiscondition as soon as possible. Some signs and symptoms include:
Bowel or bladder incontinence
Decrease in strength of legs or feet
Deformity of the legs or hips
Loss of reflexes and sensation in the legs
Stumbling or walking changes
Leg or back pain
Curvature of the spine
Skin abnormalities
What is the treatment for Tethered Cord?
Patients suspected of having tethered cord may go through the following stepsfor evaluation and treatment:
MRI of the spine
Bladder function evaluation
Somatosensory evoked potentials and Nerve Conduction Studies-to evaluate nerves and electrical impulse transmissions through the spinal cord
Surgery
It is important that a neurosurgical assessment is made asearly as possible after the onset of symptoms. In children, early surgery isrecommended to prevent further neurological deterioration. The care of patientswith tethered cord is very complex and is therefore best handled by pediatricneurosurgeons trained in treating the tethered cord syndrome. The main purposeof the surgery is to stop any further deterioration of neurological function.The surgery (Detether) the spinal cord also may restore some function or alleviate other symptoms .
What is the prognosis?
With treatment, individuals with tethered spinal cord syndrome have anormal life expectancy unless bladder and Bowel is involved.
After the initial repair, patients need close follow-up by a coordinated teamof physicians, nurses, and therapists. They may need to be treated forhydrocephalus, urologic symptoms, scoliosis, tethered cord, or muscle weakness.The exact needs of each patient depends on the type and spinal cord level oftheir Spina Bifida, making coordination between different members of the SpinaBifida team essential in tailoring the best treatment for each unique patient
Myelomeningocele / Spina Bifida
Spina bifida or myelomeningocele is a condition that occurs when the spinalcord fails to fully form early in development (in the womb, before most womenknow they are pregnant). Myelomeningocele is one of the most common birthdefects of the nervous system. It is a neural tube defect in which the skin ,muscle and bones of the spine do not completely formed. This allows the spinalcord and meninges (the membranes covering the spinal cord) to protrude out ofthe child's back. The spinal cord is exposed through the opening in the spine,resulting in partial or complete paralysis of the parts of the body below thespinal opening. The affected individual may be unable to walk and may havebowel and urinary dysfunction.
Causes
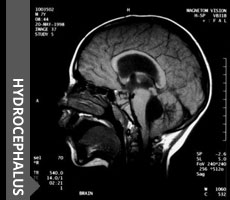
Cause of myelomeningocele is unknown. However, folic acid deficiency is thoughtto play a part in neural tube defects. Also, if a child is born withmyelomeningocele, subsequent children in that family have a higher risk thanthe general population. A viral cause or trigger has been theorized becausethere is a higher incidence of the defect in children born in the early wintermonths. Research also indicates possible environmental factors such as radiation.Other congenital disorders may also be present in the child, usually disordersof the spinal cord or the musculoskeletal system such as hydrocephalus (whichmay effect as many as 90% of children with myelomeningocele), syringomyelia,hip dislocation, or similar disorders. With the use of folate supplementationin maternal vitamins, the incidence of spina bifida has decreased dramatically.Women who are considering getting pregnant should ask their doctors about amaternal vitamin which contains folate.
Symptoms
The malformed spinal cord is open and visible through the skin of the back.This condition requires treatment within the first few days of life and iscommonly associated with hydrocephalus. Spina bifida is also associated withother problems of the brain and spinal cord such as Chiari malformations. Symptomsinclude partial or complete paralysis of the legs, with partial or completelack of sensation, and may include loss of bladder or bowel control. Theexposed spinal cord is susceptible to infection (meningitis).Visible sac-likeprotrusion on the mid to lower back of a newborn (not translucent when a lightis shone from behind the sac) Weakness of the hips, legs, or feet of a newborn.Myelomeningocele is a visible defect after the child is born. Neurologic examinationmay indicate loss of neurologic functions below the defect. For example,response of the infant to pinpricks at various locations may indicate the levelwhere sensation is maintained.
Diagnosis
Spine X-Rays may reveal the exact extent and location of thedefect
Spine ultrasound may show an abnormal spinal cord or spine
Spine CT or Spine MRI are occasionally used todetermine the location and extent of the defect.
Treatment
The goals of initial treatment are to reduce the amount ofneurologic damage caused by the defect, to minimize complications such asinfection, and to aid the family in coping with the disorder. Follow-upneurological testing as the child gets older helps to guide rehabilitation.Early surgical repair of the defect is usually recommended, although surgicalrepair may be performed later to allow the infant to tolerate the procedurebetter. Currently there are centers attempting experimental in utero surgicalrepair of spina bifida (surgical repair of the defect while the fetus is stilldeveloping in the uterus).
Before surgery, the infant must be handled carefully to reduce damage to theexposed spinal cord. This may include positioning, protective devices, andmodifications in the methods of handling, feeding, bathing and caring for theinfant.
Orthopedic intervention or physical therapy may be needed to treatmusculoskeletal symptoms. Other neurologic losses are treated according to thetype and extent of the loss of function. The goal of these interventions is tominimize future disability and maximize functioning. Surgical CSF diversion shuntingmight be needed to correct hydrocephalus.Children with spina bifida arefollowed at Spina Bifida Clinic
Lipomas and Lipomyelomeningoceles
Spinal cord lipomas are a fatty mass or tumor within the spinal cord and areusually associated with spina bifida but will, in rare circumstances occuramong adult men and women who do not have spina bifida. Lipomyelomeningoceles,congenital lesions due to the failure of closure of spinal bones associatedwith spina bifida.
Symptoms
A gradual stretching of the spinal cord causes numbness or tingling for thepatient. In extreme cases, there is weakness, difficulty in urination or bowelmovements, incontinence and stiffness of the extremities. Identified byabnormal fat accumulation that starts below the level of the skin and extendsthrough the bony opening to the spinal cord, more than 90 percent of patientswill have an obvious soft tissue swelling over the spine in the lumbosacralregion. While not painful, patients can lose neurological function over a broadrange of time. Typical neurological symptoms for adolescents and adults areweakness and bladder and bowel incontinence. Pain may be the force behindseeking treatment.
Diagnosing and Treating Spinal Cord Lipomas and Lipomyelomeningoceles
MRI's give exceptional anatomical details and can help surgeons plan theoperative procedure. Conventional x-rays will show spina bifida in most cases.
Surgical treatment is indicated at six months of age or at the time ofdiagnosis if the patient is older. The goals of surgery are to release theattachment of the fat to the spinal cord and reduce the bulk of the fatty tumorthrough a laminectomy .
Dermal Sinus Tract
A Congenital Dermal Sinus is a tract lined by stratified squamous epitheliumfound in, or very near, the midline anywhere from the nasal bridge to thecoccyx (tailbone). The tract may end just below the skin surface or may extendto the conus medullaris (part of the spinal cord) or the central canal of thespinal cord from the back, the fourth ventricle from the occipital region, orthe crista galli from the nasal bridge.
Symptoms
A Spinal Dermal Sinus may appear as a dimple or a sinus (open tract), with orwithout hairs, usually very close to the midline, with an opening of only 1-2millimeters. The surrounding skin may be normal, pigmented, or distorted by anunderlying mass. These tracts are a potential pathway for intraduralinfections, which may result in meningitis and/or an abscess. The contents ofthe dermal sinus causing sterile (chemical) meningitis may also irritate thesuperficial skin. If the tract expands into the thecal sac (the sac thatcontains the spinal cord) to form a cyst, the mass may present as a tetheredcord. In these circumstances bladder dysfunction is usually the firstmanifestation.
Diagnosis
If the tract is seen initially following birth, a MRI should be obtained. MRIalso shows masses within the canal.
Treatment
Sinuses above the lumbosacral region should be surgically removed. Althoughapproximately 25% of presumed sacral sinuses seen at birth will regress to adeep dimple on follow-up, it is recommended that all dermal sinuses should besurgically explored and fully excised prior to the development of neurologic deficitor signs of infection. The results following intradural infection are never asgood as when undertaken prior to infection. Sinuses that terminate on the tipof the coccyx rarely penetrate the dura, and may not need to be treated unlesslocal infection occurs.
Diastematomyelia - Split Cord Malformation
Split cordmalformation (Diastematomyelia) is a complex congenital condition where thespinal cord is split into two halves, each half usually functioning normally.The split is in a plane running front to back. The split in the cord can occurat any level and the split cords may reunite or not at some point below thesplit. Occasionally there is no obvious cause of the split but usually there isbone, cartilage or fibrous tissue that is between the two halves of the spinalcord. The presence of the tissue splitting the spinal cord causes tethering.The surgical procedure is to remove any tissue that is between the two splitcords, thus releasing any tethering that is present.
What are the symptoms?
The signs and symptoms of Diastematomyelia may appear at any time of life,although females are affected much more commonly than males. Pain is the numberone reason patients will visit their doctor for this problem. Other commonsymptoms include a decrease in strength of the legs; loss of bowel and bladdercontrol; sexual dysfunction; deformity of the legs, feet or hips; back or legpain; loss of reflexes and sensation in the legs; and curvature of the spine.Often there are skin abnormalities overlying the tethered cord such as midlinedimples, sinuses or tracts leading from the skin toward the spinal cord,birthmarks, fatty lumps, or small tufts of hair.
What is the prognosis?
The presence of Diastematomyelia has no influence on the prognosis when spinabifida is present. When diastematomyelia presents as a closed neural tubedefect, the prognosis for neurological function may be enhanced by earlysurgical removal of the septum, dural reconstruction into a single tube,excision of associated developmental masses and division of the tetheringfilum.
Click to know more about neurological disorders and diseases and it's treatment.






© 2016 ChildNeuroSurgeon.com. All rights reserved | Design by MHI