Case: Lipoma of Spinal Cord
Category: Spinal Dysraphism
Case Report
45days male swelling on back, soft noncystic does not increase on crying, not marked increase since birth, skin over lesion normal, moving both lower limbs well, anus non patulous.
Images

soft swelling at back
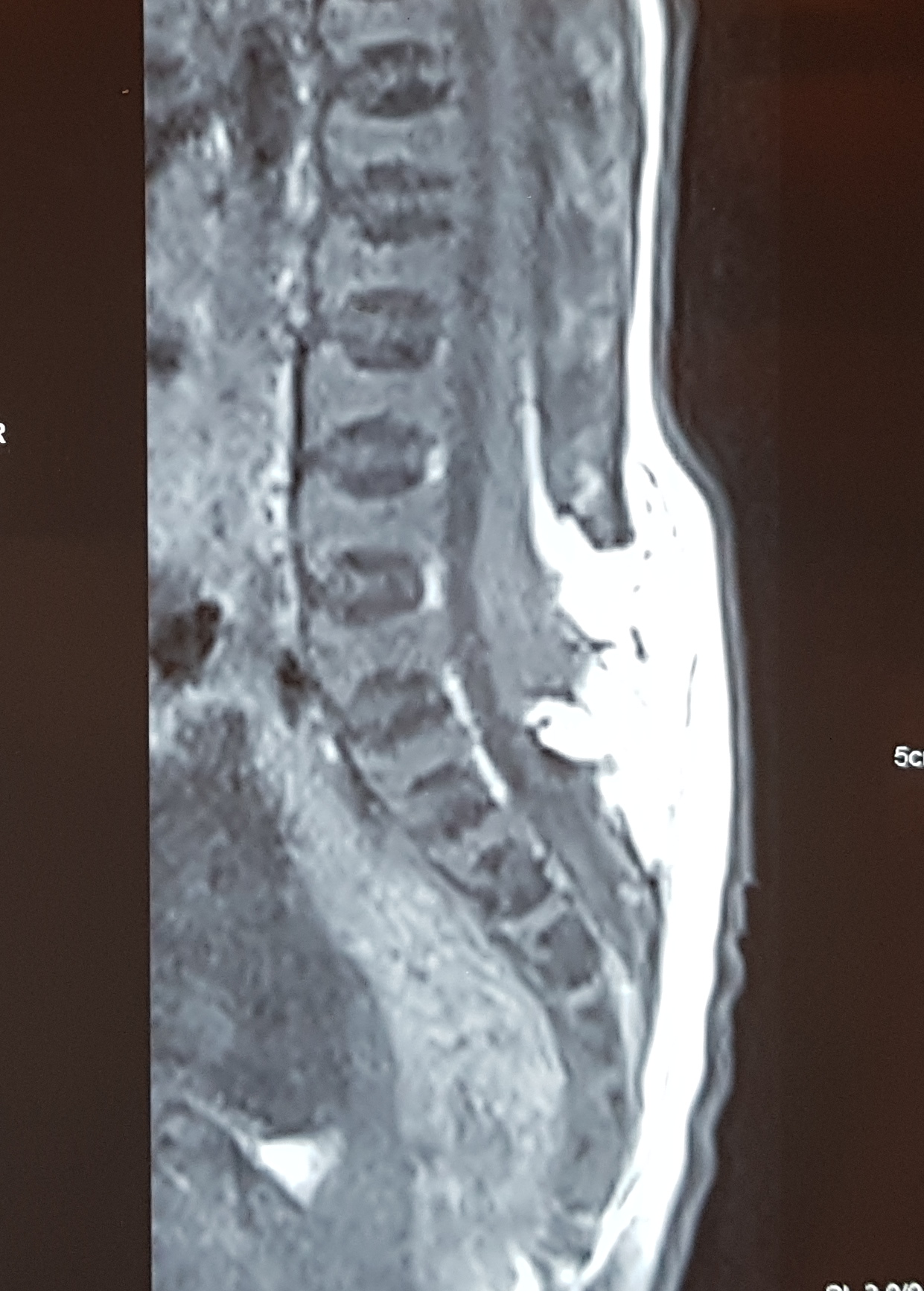
Mri shows there is absent posterior arch elements L45S1 subcutaneous lipoma attached to spinal cord and extending upto L2, low lying conus with Tethered Cord Syndrome
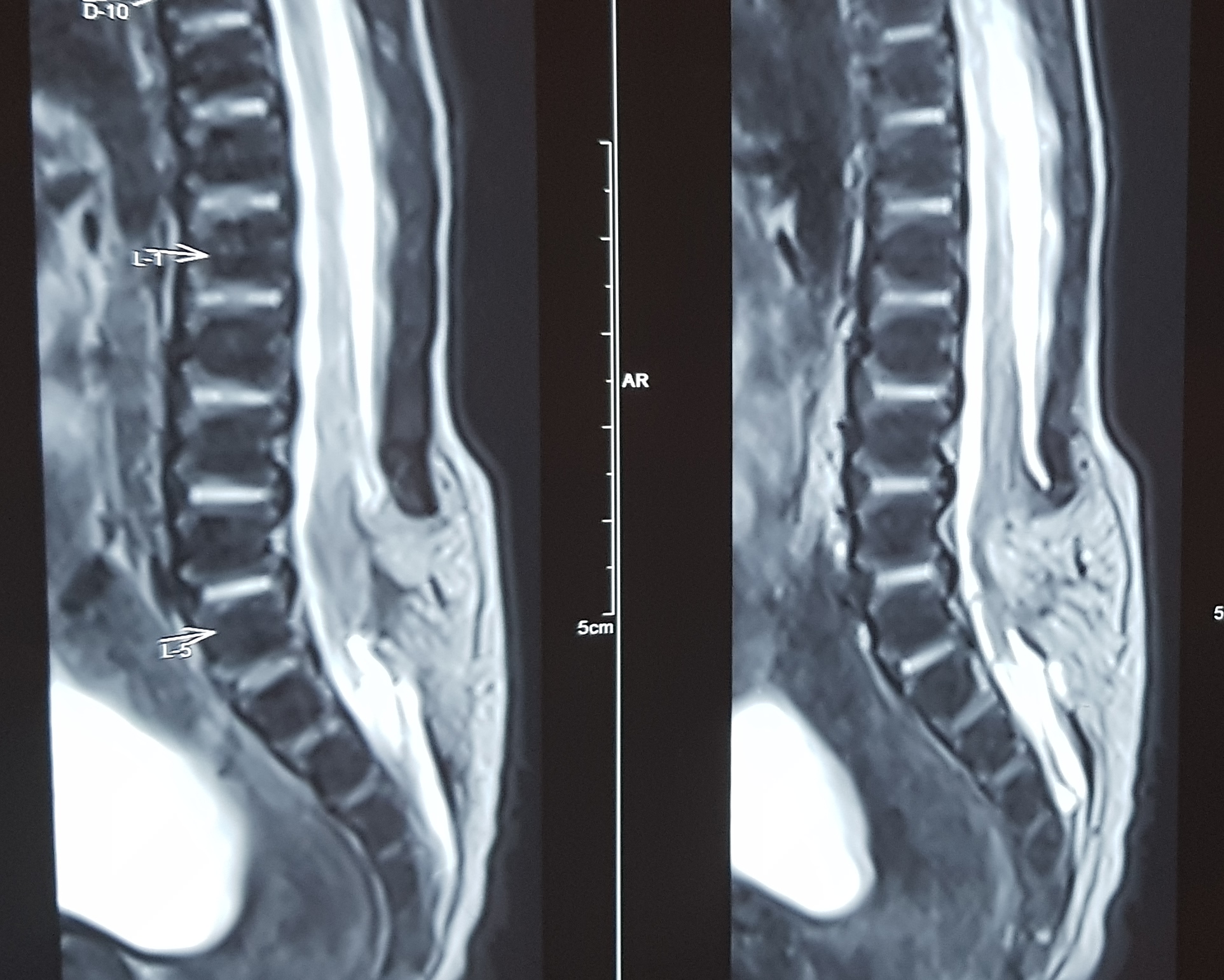
Mri shows there is absent posterior arch elements L45S1 subcutaneous lipoma attached to spinal cord and extending upto L2, low lying conus with Tethered Cord Syndrome
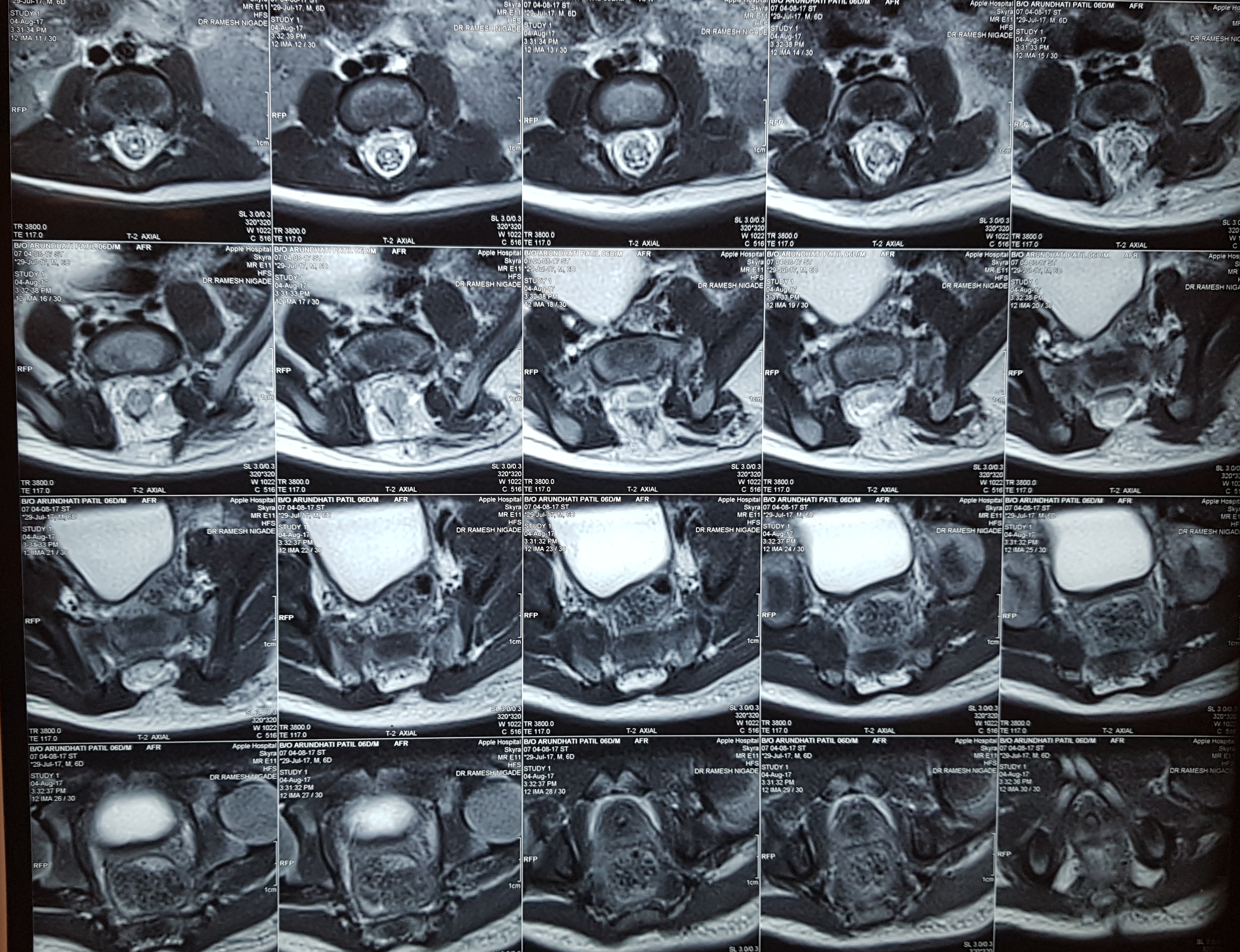
Mri shows there is absent posterior arch elements L45S1 subcutaneous lipoma attached to spinal cord and extending upto L2, low lying conus with Tethered Cord Syndrome
Description
1 No need to investigate with MRI in neonatal period if the skin is healthy and no neurological deficit
2 No need of local USG since its operator dependent and even when the lesion is picked up we still do MRI Scan . X-rays would just tell about the spina bifida it does not tell about the intradural patholgy . Ct scan is inferior in detecting the pathology and also exposes the child to radiation So Mri Remains the investigation of choice ideal if I see a child before 1 months we get MRI by 4-5 Months age . we need to reassure the parents no harm happens while waiting.
3 Neonatal MRI is potentially dangerous for child (hypothermia) if we r not intervening if skin is healthy. When we intervene at 6 months then might be interval change and need to repeat the MRI also
4What's ideal age to detether?
5When the child starts sitting with support and without support is the time when the spinal cord starts taking the irreversible damage due to the movements of the trunk. so elective detethering to be done by 6 months
6 Detethering surgery is a major undertaking and child has to be fit to undergo surgery lasting more than two hour, blood loss . also during the post op period is CSF leak happens the child should have enough reserve to come out of the same so we wait till 6 months or atleast 7kgs
7In a child without deficit, if appropriate surgery is done there is little risk of post-op deficit.
Moral of the Story
1
In addition to excision of lipoma, one require division of filum terminale and lysis of adhesions between cord and dura to complete the detethering surgery rather than excision of the subcutaneous lipoma.
2
These children almost never develop hydrocephalus post-op, rarely have hydrocephalus pre-op. Without clinical suspicion ,it is not necessary to do MRI of head . also there is no chiari herniation in lipomeningomyelcocole since the embryologically the defect happens in secondary neurulation and meninigomyelocole is defect that happens is primary neurulation